
Tags
3 Percent Rule, Appetite-suppressing drugs, BMI, Calorie Deficit Principle, GLP-1, GLP-1 side effects, Glucagon, Healthy diet, How to lose weight naturally, Mounjaro, Obesity, Obesity causes, Ozempic, Wegovy

Introduction
In recent years, the use of appetite-suppressing Glucagon-Like Peptide-1 (GLP-1) drugs—such as Mounjaro, Wegovy, and Ozempic—has surged. Originally developed to help people with type 2 diabetes regulate blood sugar, these drugs now dominate the weight loss conversation. But at what cost—physiologically, financially, and socially?
Let’s explore the alternatives and ask whether these drugs are truly necessary for most people.
Understanding Glucagon and GLP-1 Drugs
Glucagon is a hormone produced by the pancreas that helps regulate blood glucose levels. It plays a vital role in natural weight control by:
- Promoting fat burning
- Increasing energy expenditure
- Enhancing metabolic flexibility (switching between glucose and fat as fuel)
- Suppressing hunger signals from the brain’s hypothalamus, the region that maintains the body’s balance between hunger, thirst, temperature, sleep and emotions
GLP-1 drugs mimic this hormone’s effects—but artificially, and not without side effects.
What Causes Obesity?
Medically, obesity is defined as having a Body Mass Index (BMI) over 30. It can arise from:
- Medical conditions: Usually caused by hypothyroidism or polycystic ovary syndrome, and, more rarely, by Cushing’s syndrome, insulinoma, genetic syndromes, depression, and certain medications
- Non-medical factors: Overeating, poor diet quality, sedentary lifestyle, stress, emotional eating, and food marketing
While estimates vary, less than 5% of obesity cases are considered to be due to medical conditions. The remaining 95% stem from behavioural, environmental, and societal influences.
Quite simply: most obese individuals are not metabolically broken—they’re caught in a system that promotes overeating and inactivity.
Three Paths Forward
Faced with obesity, people typically consider three options:
- Do nothing and accept the consequences
- Take GLP-1 drugs to suppress appetite and lose weight
- Adopt a healthier diet and exercise routine
Let’s examine the second and third options more closely.
Option 2: Take the Drugs
GLP-1 drugs can lead to rapid weight loss—but not without consequences.
Common Side Effects:
- Gastrointestinal: Nausea, vomiting, diarrhoea, constipation
- Neurological: Headaches, dizziness, sleep disturbances
- Endocrine/Metabolic: Increased pancreatic enzymes, low blood pressure
- Musculoskeletal: Tendinitis, arthritis
- Renal: Kidney stones
- Reproductive (Women): Vaginal dryness, sagging labia (“Ozempic vulva”)
- Other Serious Risks: Doubled risk of pancreatitis
Financial Cost: Manufacturer Eli Lilly recently raised the price of Mounjaro by 170%. In the UK, the highest dose now costs £330/month, discounted to £247.50 for suppliers. Estimates vary on how long it takes to lose up to 20% of your body weight with Mounjaro, but it could be anywhere between 8 and 18 months. Even with marked-up pharmacy discounts, a private customer might pay £3,267 per year. It’s not a cheap way of losing weight!
What Happens When You Stop? Unless you’ve changed your diet and exercise habits while taking the drug, the effects reverse quickly when you stop:
- Some, or all of the weight will come back
- Appetite and cravings will return—often stronger than before
- Metabolic markers (blood sugar, cholesterol, inflammation) will rebound to previous levels
- Emotional toll: frustration, anxiety, loss of self-esteem
Without diet and exercise lifestyle changes, the drug is a temporary fix with a high price tag, which begs the question: why not make these lifestyle changes immediately and let nature take its course?

Bert and Mavis cartoon.
For more Bert and Mavis cartoons, see Bert and Mavis: The First Fifty Cartoons
Option 3: Change Your Lifestyle
This is where it gets personal—because it’s exactly what I did.
In October 2024, my doctor diagnosed hypertension. I weighed 109 kg, with a BMI of 32.9—clinically obese. I was prescribed a calcium channel blocker to relax and widen my blood vessels, thus reducing my blood pressure. That diagnosis and prescription stopped me in my tracks. As a former engineer, I reasoned: why treat the symptom when I could remove the cause? I decided to lose weight.
Losing Weight: The Calorie Deficit Principle
In simple terms, if you consume more calories than the body needs to maintain a stable weight (the maintenance level), the extra calories are deposited as fat. If by employing dietary constraints and exercise, you burn more calories than the maintenance level, your body will call upon the fat deposits to make up the deficit. You will lose weight. In this context, a rule of thumb is:
A 555-calorie deficit per day equals 0.5 kg weight loss over a week.
(You may see this rule written as a 500-calorie deficit per day equals 1 lb weight loss over a week. It’s the same rule.)
Weight loss isn’t magic—it’s maths.
The 3 Percent Rule—A Simple Guide to Smarter Eating
To assist my revised eating and drinking habits, I created an easy-to-follow fat and sugar content rule to apply to the food and beverage I consumed:
Eat nothing containing more than 3% fat, 3% sugar, no ultra-processed foods, and no alcohol.

Why 3%? After examining the calorie content of foods that had contributed to my weight gain—cake, cheese, ice cream, chocolate, biscuits, crisps, sweets, red meat, wine, beer—I realised they were all high in fat or sugar. The 3% threshold eliminated them naturally. (I liken my 3% rule to other simple benchmarks that work: walking 10,000 steps a day, drinking 2 litres of water a day.)
The 3 percent rule steers you toward:
- Fresh and dried fruit
- Nuts and seeds
- A variety of salad ingredients and fresh vegetables
- White meat (fish, chicken, some pork)
- Water, tea, coffee, and other sugar-free liquids
- Limited bread, rice, potatoes, or pasta
- No alcoholic beverages
This is a diet rich in proteins, vitamins, minerals and also contains some fats, fibre and carbohydrates, all of which the body needs to stay healthy
Exercise and Results
After the hypertension diagnosis in October 2024, I reset my diet and restarted daily walks—beginning at 3 km/day and building up to 10 km/day, five days a week. By May 2025, I had lost 25 kg, averaging 1 kg per week; a 23% loss of my initial body weight.
My Weight Loss Journey—November 2024 to May 2025
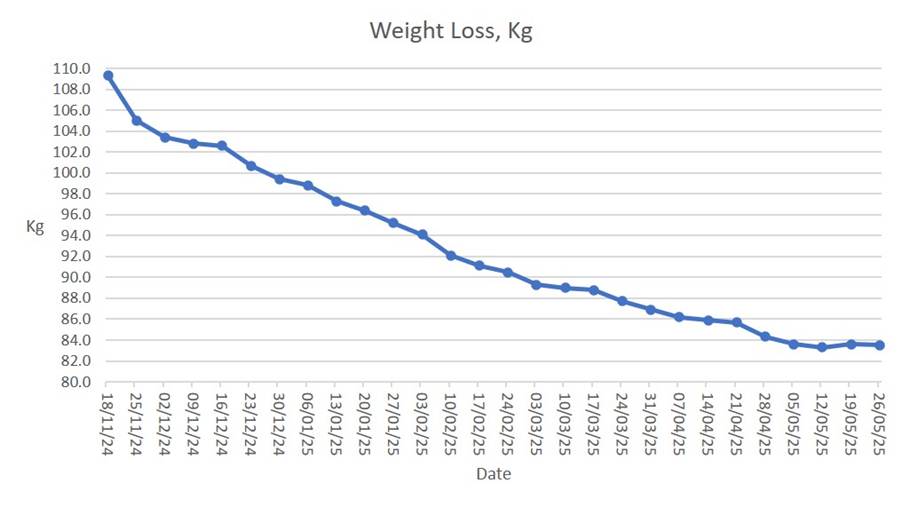
Now, in September 2025, I walk up to 13 km/day. My weight is stable at 83 kg, and my blood pressure has normalised. My doctor agreed I could stop taking the calcium channel blocker. This transformation has cost me a new waterproof shell walking jacket, a better-fitting day rucksack, and a new pair of walking boots. Compare that to the £3,267 annual cost of Mounjaro. I’ll take the boots!
Motivation and Momentum
I understand why some people turn to GLP-1 drugs for a boost. But look at my graph: I lost 6 kg in the first three weeks—nearly a stone. That early success boosted my morale and kept me going.
Conclusion
All it takes to lose weight is:
- The ability to read and understand food nutrition labels
- Simple calorie-in, calorie-out maths
- A pair of walking boots (or a gym membership)
- Sensible motivation (mine was high blood pressure)
- Support from family
- And lots of willpower
Try it—and enjoy buying slimmer clothes.
Listen to Your Body—With a Wink
“Listen to Your Body… Unless your body says you can have more ice cream.”
August 2025
Yes, that’s me in the photo. After months of walking, label-reading, and resisting temptation, I’ve earned the right to wear the shirt and hold the spoon.
Acknowledgement
I’m indebted to Microsoft’s generative AI chatbot, Copilot, for much of the background research necessary to write this article. I verified the findings and followed up on the references. I found no discrepancies, inconsistencies, or inaccuracies.
Bibliography
- NHS: Causes of Obesity
- Health Survey for England 2022
- UK Government Obesity Profile
- Ben Bennetts: The Perils of Daily Pill-Popping
- Mounjaro vs Wegovy: Cost and Side Effects
- Diabetes.co.uk: GLP-1 Side Effects Study
- LADBible: Ozempic Vulva and Daily Changes
- BBC News: GLP-1 Drug Trends
- TryHabitual: Mounjaro Week-by-Week Guide
- The Calorie, Carb, and Fat Bible 2022
(^_^)
